
What is Alexithymia?
Alexithymia is a difficulty identifying, interpreting, and describing emotions, sometimes described as emotional blindness. In the research literature, the construct is usually organized around three core factors: difficulty identifying feelings, difficulty describing feelings, and an externally oriented thinking style that focuses more on facts, events, or practical tasks than on inner experience.[1][2] In plain language, a person may notice that something is wrong: perhaps sense some tension, agitation, heaviness, shutdown, or physical activation, but without being able to answer the question, “How do you feel?”
The word alexithymia literally means “no words for emotions,” and that bluntly captures the gist of the problem. The concept came out of the psychosomatic field in the early 1970s, when clinicians kept seeing patients whose distress showed up more through the body and behavior than through clear emotional language.[19]
Interoception: how emotions show experientially
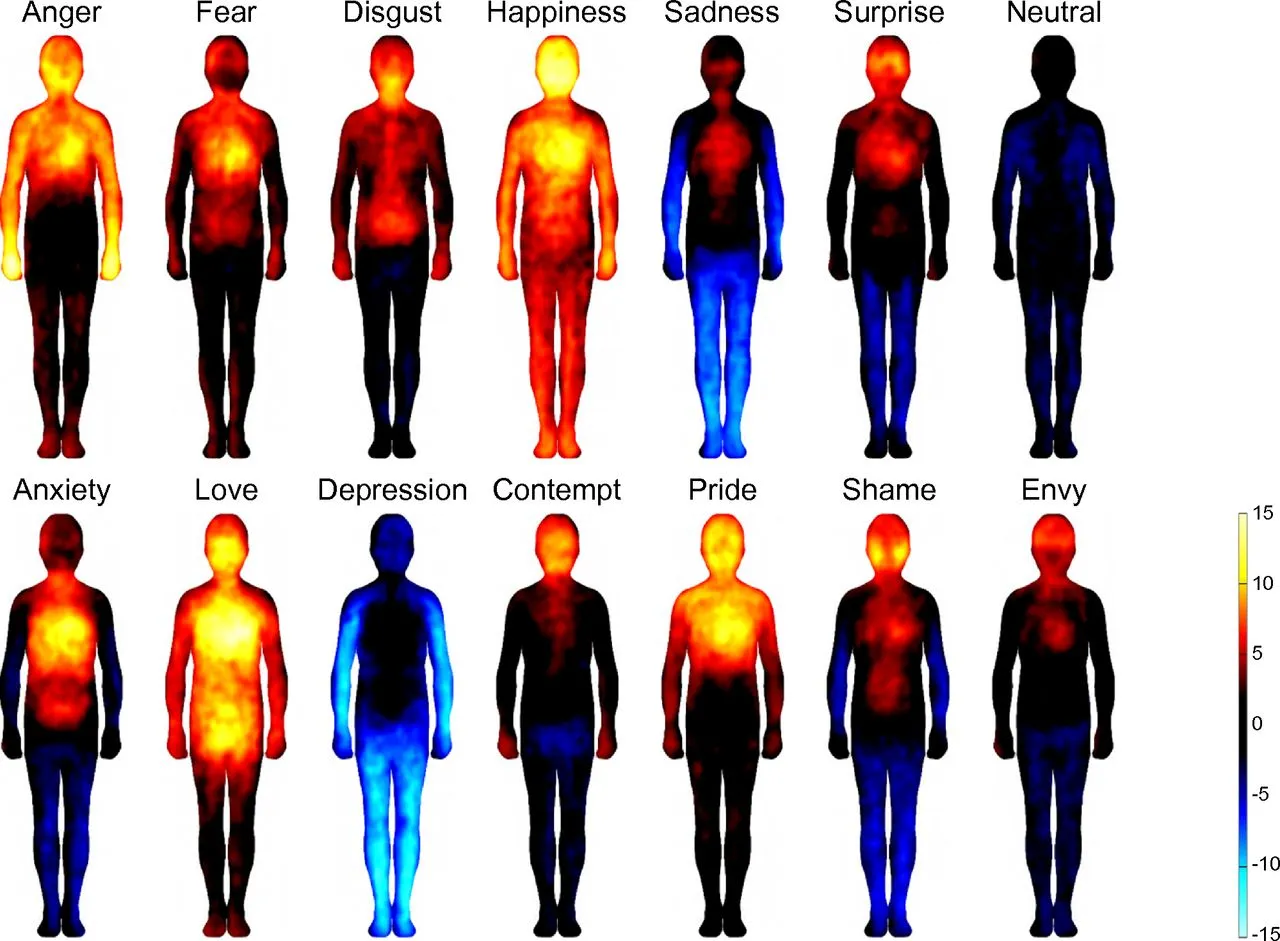
Most people do not recognize emotions by abstract introspection. They feel and recognize them viscerally by reading body signals in context: breath, muscle tension, heartbeat, stomach sensation, heat, posture, agitation, pressure, and urge. That process is called interoception, and it is one of the foundations of emotional awareness. When interoception is weak or dysregulated, people are effectively flying blind. They may feel broad activation, but don’t understand what it means.[1][13]
That does not mean the person has no emotions. Many people with alexithymia feel emotions intensely. The problem is usually understanding, not absence. The signal is there, but it is hard to decode quickly enough to guide decision-making, communication, or self-regulation. That is why alexithymia often looks paradoxical from the outside: someone can care deeply, react strongly, or become overwhelmed, while still struggling to name and express what they feel.
What alexithymia is not
Alexithymia is currently not a defined standalone diagnosis, and it is not the same thing as emotional numbness, repression, apathy, or an unwillingness to talk about feelings.[1] Those states can and often do overlap, but they are not identical. A person who is repressing emotion often has at least partial access to what they feel and is holding it back. A person with alexithymia often has a more basic problem - the emotion is poorly differentiated or not translated into usable language in the first place.
It is also a mistake to equate alexithymia with coldness or lack of empathy by default. Relationship problems can happen because needs, boundaries, and emotional cues are hard to identify and communicate, not because the person does not care. Many people spend years being told they are detached, avoidant, or uninterested when the more accurate problem is that their inner experience is not accessible enough to communicate clearly.
How researchers describe it today
Older models of alexithymia sometimes emphasized a limited fantasy life or reduced imagination. Newer work is more careful. Contemporary researchers usually focus on the appraisal and language side of emotion, and newer tools also distinguish between difficulties with negative emotions and difficulties with positive emotions.[1][15] This means that two people can both score high on alexithymia while presenting differently. One may feel chronic distress but be unable to label it precisely. Another may function well in daily life but struggle to register subtle satisfaction, affection, pride, or relief.
Primary vs. secondary alexithymia
A common practical distinction is between primary and secondary alexithymia. Primary alexithymia usually refers to a more longstanding, trait-like emotional processing style. Secondary alexithymia refers to a pattern that appears or worsens in response to trauma, chronic stress, depression, burnout, or neurological illness. A related term, acquired alexithymia, is often used more specifically for alexithymia that appears after traumatic brain injury or neurological disease, including conditions such as Parkinson’s disease. The boundary between these categories is not always clean, but the distinction is useful because it reminds clinicians to ask whether the problem is deeply longstanding, more acquired, or some mixture of both.[1][17]
Signs and Symptoms
Alexithymia often shows up in ways that are easy to misread. From the outside, someone may look analytical, detached, indecisive, concrete, or difficult to reach emotionally. Internally, the experience is often less calm than it appears. Many people feel overloaded, blank, confused, flooded, or stuck with only broad labels like bad, stressed, weird, or overwhelmed. What to look out for:
- Always drawing a blank when asked how you feel.
- Struggling to tell similar emotions apart, such as anxiety versus excitement, guilt versus shame, or sadness versus emptiness.
- Talking about events, facts, or theories instead of internal experience.
- Having strong bodily sensations without a clear emotional label.
- Finding decisions unusually difficult because feelings do not become usable signals.
- Realizing what you felt only hours, days, or sometimes even weeks later, after the moment has passed.
- Defaulting to analysis, work, distraction, scrolling, food, or substances when something feels “off” but unclear.
- Feeling misunderstood in therapy or relationships because your inner state does not translate into words quickly enough.
- Sometimes struggling to interpret other people’s emotional cues, especially when tone, facial expression, and context are subtle or mixed.
- Using a small set of vague labels such as fine, tired, stressed, or numb to cover a wide range of experiences.
Real-life examples
In real life, alexithymia can look surprisingly ordinary. Someone may keep saying “I don’t know” in a relationship conflict because they genuinely cannot tell whether they feel hurt, ashamed, angry, or overwhelmed. They may notice a racing heart before a social event but only later realize it was anxiety. They may also struggle with preference-based decisions because emotions are part of how people usually know what they want, what feels off, and what matters.
How alexithymia can feel from the inside
One of the most frustrating parts of alexithymia is that the person often knows something is happening. There may be tightness in the chest, a sinking feeling, irritability, stomach discomfort, shutdown, or mental noise. What is missing is the bridge from sensation to meaning. Instead of anger, grief, shame, relief, envy, or affection, there is just an uncomfortable signal that does not resolve into a clear interpretation. That often produces secondary anxiety because not knowing what you feel makes it harder to know what you need.
How it shows up around other people
In relationships, alexithymia often leads to late or incomplete emotional communication. Needs are not expressed until they become crises. Conflict is processed intellectually rather than emotionally. Affection may be felt but not verbalized. Similar patterns can show up in therapy, where open-ended questions like “What are you feeling right now?” may produce silence, guessing, or frustration instead of insight.[11][12]
How Common Is Alexithymia?
Alexithymia is common in the general population and dramatically more common in high-burden groups. Severe alexithymia affects roughly 1 in 10 people, and among people with diagnosed mental disorders the prevalence can rise toward half of treatment populations.[1][3] Once you look across the literature, alexithymia stops looking niche and starts looking like a hidden layer running through large parts of the health system.
Across published studies, the broader prevalence picture is clear. Exact numbers vary by population, method, and cutoff, but the direction is unequivocal: alexithymia clusters wherever emotional distress, somatic burden, and treatment complexity are already high.
| Population or condition | Reported prevalence | Comparison context |
|---|---|---|
| General population | Roughly 10% | Useful baseline for severe alexithymia in population samples.[1][3] |
| Psychosomatic disorders | 40%-60% | High-burden somatic clinical group.[17] |
| Anxiety disorders | 13%-58% | Wide range across diagnosis, sample, and cutoff.[17] |
| Depressive disorders | 32%-51% | Consistent with the strong alexithymia-depression association.[8] |
| Eating disorders | 24%-77% | Often elevated across eating-disorder samples.[7] |
| Addictive disorders | 30%-50% | Elevated across substance-use samples.[6] |
| Post-traumatic stress disorder (PTSD) | Up to 75% | Reported in war-veteran PTSD samples.[28] |
| Borderline personality disorder (BPD) | Up to 62% | Reported in adolescent BPD samples.[29] |
| Bipolar disorders | 27% | Reported in bipolar-spectrum comparison work.[30] |
| Schizophrenia | 30%-46% | Reported in stable schizophrenia samples.[31] |
| Obsessive-compulsive disorder (OCD) | 11%-36% | Lower than some psychiatric groups, but still often elevated.[17] |
| Attention deficit hyperactivity disorder (ADHD) | 42% | Reported in an adult ADHD clinical sample.[5] |
| Autism spectrum disorder (ASD) | 50% | Meta-analytic estimate across autistic samples.[4] |
| Epilepsy | 26%-76% | Reported across epilepsy studies in a seizure-disorder review.[32] |
| Psychogenic non-epileptic seizures (PNES) | 30%-90% | Often higher than epilepsy samples in the same review literature.[32] |
| Traumatic brain injuries (TBI) | 30%-60% | Reported in neurological-disease literature.[17] |
| HIV/AIDS | 36% | Reported in a cross-sectional sample of people living with HIV/AIDS.[33] |
| Type 2 diabetes | 43% | Meta-analytic estimate in type 2 diabetes samples.[34] |
| Systemic lupus erythematosus | 56% | Reported in a Brazilian cross-sectional sample.[35] |
| Multiple sclerosis | 53% | Reported in recent multiple-sclerosis literature.[36] |
| Rheumatoid and psoriatic arthritis | 39% | Reported in a cross-sectional rheumatology sample.[37] |
| Transgender people | 32% | Reported in autistic and nonautistic transgender adults.[38] |
Why Alexithymia Matters
Alexithymia matters because emotional awareness is not an optional nice-to-have. It is infrastructure for self-regulation, relationships, therapy, decision-making, and wellness overall. When that infrastructure is weak, stress stays unprocessed and accumulates, needs stay unnamed, conflict resolution happens later than it should, and distress gets routed into behavior, symptoms, or shutdown instead of becoming something usable.[1]
Mental health and therapy
Across the literature, alexithymia consistently amplifies burden across disorders. It is strongly associated with depressive symptoms, and meta-analytic work shows that link is not trivial or incidental.[8] A separate systematic review and meta-analysis found alexithymia is also associated with suicide ideation and behavior.[9]
“Alexithymia is widely seen as a risk factor for psychopathology, and is thus of high clinical interest.”[40]
David A. Preece, PhD - Associate Professor of Psychology at Curtin University and James J. Gross, PhD - Professor of Psychology at Stanford University
Therapy is another major reason alexithymia is important. Many treatment models assume clients can observe emotions in real time and put them into words. If that assumption is wrong, even a motivated client can look resistant, defended, or “not doing the work.” Reviews and clinical studies link alexithymia with weaker therapeutic alliance and poorer psychotherapy outcomes, especially when treatment stays highly verbal and insight-driven without enough structure.[11][12]
“If I had a dollar for every time a therapist asked me, ‘How did that make you feel?’ and I had no clue at all, I’d be rich enough by now to hire a full-time assistant to express emotions for me.”[41]
@violetxoxox
Relationships, work, and daily decisions
In everyday life, alexithymia creates friction anywhere emotional information is supposed to motivate and guide behavior. People may stay too long in situations that are draining because they do not recognize resentment or exhaustion early enough. They may struggle to set boundaries because they detect overload only after it becomes extra intense. Motivation can also become harder to trust: if desire, boredom, dread, pride, or relief do not register clearly, it becomes harder to know what to start, stop, pursue, or protect. They may seem cold and emotionally unavailable in relationships even while caring deeply. They may also rely too heavily on logic for decisions that require values, preference, desire, or intuition.
”Not being able to read your emotions is so much more than just not knowing how you feel, it’s making major life decisions without being able to use your emotions as a guide.”[42]
Sudden_Silver2095
”Alexithymia has been associated with problems with motivation and finding direction and purpose in life.”[43]
Dr. Alok Kanojia
Physical symptoms and health behavior
Alexithymia does not stop at mental health - it changes how distress is carried in the body. A systematic review and meta-analysis in chronic pain found robust links between alexithymia and greater pain intensity, physical interference, depression, and anxiety.[10] When emotional signals stay unread for too long, the body becomes the loudest channel left. Substance use follows a similar logic: when people cannot identify what they feel or what would regulate it, fast-acting external regulators become more attractive.[6]
When emotions become symptoms
Alexithymia also helps explain why distress so often shows up as symptoms instead of clearly labeled feelings. A classic quantitative review found a meaningful association between alexithymia and somatization.[26] Research on functional gastrointestinal disorders points in the same direction: when emotions are difficult to identify, internal arousal is more likely to be experienced as diffuse physical discomfort, symptom monitoring, and alarm.[27]
Cardiovascular disease and mortality
Alexithymia reaches the cardiovascular system too. Population research links it with hypertension and subclinical atherosclerosis, and a recent systematic review argues that alexithymia belongs in the conversation about cardiac prevention rather than being dismissed as a soft personality variable.[21][22]
The longitudinal data are hard to ignore. In middle-aged men, cardiovascular death risk increased by 1.2% for every 1-point increase in alexithymia score over roughly 20 years of follow-up.[23] Separate cohort work found higher all-cause mortality risk in alexithymic men over 10 years, and community-based data now connect alexithymia with higher estimated 10-year cardiovascular risk comparable with smoking or high LDL even in otherwise healthy adults.[24][25]
The mechanism is not mysterious - unread stress becomes chronic (allostatic) load. When distress is hard to detect early, hard to regulate deliberately, and easy to somatize, the body carries the cost. That’s also why a recent review explicitly argues that assessing and treating alexithymia should be part of primary, secondary, and tertiary prevention of heart disease.[22]
Causes and Risk Factors
There is no single cause of alexithymia. It is better understood as a final common pathway that can emerge through different developmental, neurobiological, and environmental routes.[1] Two people can look similarly alexithymic on the surface while having very different histories and treatment needs.
Twin data support a meaningful genetic contribution, but the environment matters just as clearly.[20] Common pathways discussed in the literature include long-standing interoceptive and neurobiological differences, neurodevelopmental conditions, emotional environments where feelings were ignored or punished, trauma and chronic stress, and psychiatric or medical states that reduce emotional access or overload it.[1][4][5][13] Depression, eating disorders, chronic pain, substance use, and neurological conditions can all interact with alexithymic traits and make emotional processing harder.[6][7][8][10]
One social pathway is described by the normative male alexithymia hypothesis, which argues that some men’s difficulty identifying and describing emotion is shaped by masculine socialization rather than biology alone.[44] Recent work finds that masculine norms such as emotional control, self-reliance, and work primacy were associated with internalizing symptoms through alexithymia and emotion-regulation difficulties in a sample of 740 men.[45]
Why the same symptom can have different origins
This is clinically important. Someone with longstanding trait-like alexithymia may need slow, structured skill-building in interoception and emotional vocabulary. Someone whose emotional access worsened during burnout, trauma, or a major depressive episode may need those skills too, but also needs treatment for the state that is suppressing access to emotion. If the same presentation follows a neurological event or brain injury, medical evaluation becomes part of the picture.
That is why a good alexithymia assessment looks for pathway, not just score. The question is not only whether difficulty exists. It is how it developed, what maintains it, and which layer of emotional processing is most impaired.
Alexithymia and Neurodiversity
Alexithymia is often hidden inside broader neurodevelopmental labels. In autism, a meta-analysis estimated alexithymia in about half of samples, far above general-population levels.[4] That has led to the “alexithymia hypothesis”: the idea that some emotion-processing difficulties often attributed to autism may be better explained by co-occurring alexithymia.
Research on interoception supports that argument. One influential study found that impaired interoception tracked more strongly with alexithymia than with autism itself.[13] In practice, that means emotional-awareness support should not be treated as irrelevant just because autism is already recognized. The emotional access problem may still be specific, measurable, and highly trainable.
ADHD is a similar story. In one adult ADHD clinical sample, 41.5% of participants met the threshold for alexithymia.[5] That overlap can compound difficulties with impulsivity, delayed self-awareness, emotional outbursts, and decision-making. If a person already struggles with attentional control or response inhibition, poor access to emotional signals makes self-regulation harder still.
The practical takeaway is that neurodivergent people often need emotional-health tools that are more concrete, scaffolded, and body-linked than standard advice assumes. Open-ended reflection alone is often not enough. Concrete options, explicit feeling labels, examples, pattern tracking, and repeated practice usually work better.
Diagnosis and Assessment
Alexithymia is currently not a standalone DSM-5 or ICD-11 diagnosis. Researchers and clinicians usually describe it as a multidimensional trait, profile, or clinically important transdiagnostic factor that can coexist with many diagnoses or show up on its own.[1] The practical question is not only “Do you meet a threshold?” but also “Where is emotional processing breaking down, and how much does that breakdown interfere with daily life, treatment, and relationships?”
Assessment usually combines history, clinical pattern recognition, and validated measures. The classic research questionnaire is the Toronto Alexithymia Scale (TAS-20), which helped define the modern construct in a measurable way, but also has known psychometric limits.[2] Newer self-report measures such as the Perth Alexithymia Questionnaire (PAQ) were developed to separate difficulties involving positive and negative emotions and to better capture dimensions TAS-20 handle less well.[15] Interview-based tools such as the Toronto Structured Interview for Alexithymia (TSIA) can add clinical context.[14] Researchers and clinicians also used the Bermond-Vorst Alexithymia Questionnaire (BVAQ) in the past, less so now.[18]
Why self-report alone has limits
There is an obvious challenge built into alexithymia measurement: self-report asks people to describe how well they understand feelings, which is exactly the domain that may be impaired. That does not make self-report useless, but it does mean scores should be interpreted in context. Interview data, longitudinal patterns, examples from therapy, and collateral information can all improve accuracy.[1][14]
What clinicians often differentiate alexithymia from
Good assessment usually tries to separate alexithymia from emotional numbness, dissociation, severe depression, low motivation, deliberate avoidance, and social communication problems that are not fundamentally about emotional access.[1] Those states can overlap, but they are not interchangeable. Getting the formulation right is important because it changes what treatment is likely to help.
Treatment and Improvement
Alexithymia can improve. The clearest recent signal in the intervention literature is that integrative approaches work best - not one isolated technique, but a combination of psychoeducation, interoception work, emotional vocabulary building, emotion differentiation practice, and communication training.[1][16]
That makes sense clinically. If someone has trouble noticing emotion in the body, naming it precisely, and expressing it to others, treatment has to work across all three levels. Useful approaches often include:
- Teaching explicit emotion concepts instead of assuming the person already has them.
- Building body awareness and interoceptive tracking step by step.
- Practicing finer emotional distinctions instead of accepting only broad labels like good, bad, or stressed.
- Linking emotions to context, needs, values, urges, and action tendencies.
- Using structured prompts, guided journaling, worksheets, or repeated exercises that reduce the burden of generating emotion-language from scratch and on the spot.
- Making therapy slower, more concrete, and less dependent on immediate introspective fluency.
What often helps therapy work better
If therapy has felt vague or unhelpful, the issue is not always that therapy “doesn’t work.” It may be that the therapeutic approach assumes skills that alexithymia weakens. Many people do better when sessions include concrete examples, emotion lists, body-based check-ins, comparisons between similar feelings, and more time spent translating raw experience into language. Tracking patterns between sessions can help too, because alexithymic people often understand emotions more clearly with delay after the moment has passed.
”The most effective means known to humans for managing stress ranging from minor hassles to major traumas is talking about your stress with another trusted person. And if you can’t put your stress into words, if you can’t describe what you’re feeling, you’re severely handicapped.”[46]
Dr. Ronald F. Levant, EdD, ABPP, MBA, DHL (Hon), psychologist, professor emeritus, and a former president of the American Psychological Association (APA)
What usually is not enough on its own
Advice like “just journal,” “just be mindful,” or “just open up more” is often too vague. Those suggestions presuppose the very skill that is missing. Mindfulness can be valuable, but only if it is scaffolded toward noticing and naming emotion rather than remaining a generalized awareness exercise. Insight meditation practice can be valuable, but only if the person has a way to generate emotionally meaningful data in the first place.
In practice, many people do best with a blend of body-based noticing, vocabulary expansion, concrete prompts, and external supports. Some find fiction, film, drawing, or guided reflection useful because these formats externalize emotional patterns and make them easier to recognize indirectly before they can be recognized directly.
Frequently Asked Questions
Do people with alexithymia still feel emotions?
Usually yes. Alexithymia is most often a problem of recognizing, differentiating, and describing emotions, not a total absence of feeling. Many people with alexithymia feel emotions strongly but cannot decode them clearly enough to use them in real time.[1] There may also be a subgroup, often discussed in autistic samples, with very weak interoceptive signals; more research is needed to understand that distinction.[13]
Is alexithymia the same as autism?
No. Alexithymia and autism frequently co-occur, but they are distinct constructs. A large meta-analysis found very high alexithymia rates in autistic samples, yet research also suggests that some emotion-processing differences are better explained by co-occurring alexithymia than by autism alone.[4][13]
Is alexithymia the same as emotional numbness or dissociation?
No. Emotional numbness and dissociation usually involve reduced access, reduced intensity, or a sense of disconnection. Alexithymia more often involves poor interpretation and language for emotion. They can overlap, especially under trauma or severe stress, but they are not identical and should not be treated as interchangeable.[1]
Can adults improve alexithymia?
Yes. The best-supported approach is usually structured, multimodal work that improves noticing, labeling, differentiating, and expressing emotion rather than relying on one technique alone.[16]
Can alexithymia affect physical health, like blood pressure or heart disease?
It can. Research links alexithymia with hypertension, vascular risk markers, and mortality signals in men. The most likely pathway is that the body carries chronic stress load resulting from suppressing emotions, and that the related medical risk is easy to miss until it is already developed into something louder.[21][22][23][24]
How do you support someone with alexithymia?
The most helpful approach is usually to be concrete rather than push for instant emotional fluency. Specific questions, examples, feeling lists, body-based check-ins, and more time to process tend to work better than broad prompts like “just tell me how you feel.” Support also works better when it avoids moralizing the difficulty. Alexithymia is usually frustrating for the person experiencing it too.
When should someone seek professional help?
If alexithymia is significantly interfering with relationships, therapy, work, addiction recovery, chronic pain management, or safety, it is worth bringing to a clinician directly. The same is true if emotional access changed sharply after trauma, neurological illness, brain injury, or a major depressive episode.
Next Steps
If this description fits you, the most useful next step is identifying where emotional processing is breaking down, and what is the likely reason for it. Once that becomes clearer, the problem becomes much more workable.
Some people benefit from self-guided skill-building. Others benefit most from a therapist who understands alexithymia and can work in a slower, more concrete way, addressing some unhelpful beliefs about emotions. If the difficulty is severe, longstanding, or tied to trauma, depression, autism, ADHD, addiction, chronic pain, or relationship conflict, it is worth addressing directly rather than hoping it resolves as a side effect of something else.
For practical next steps:
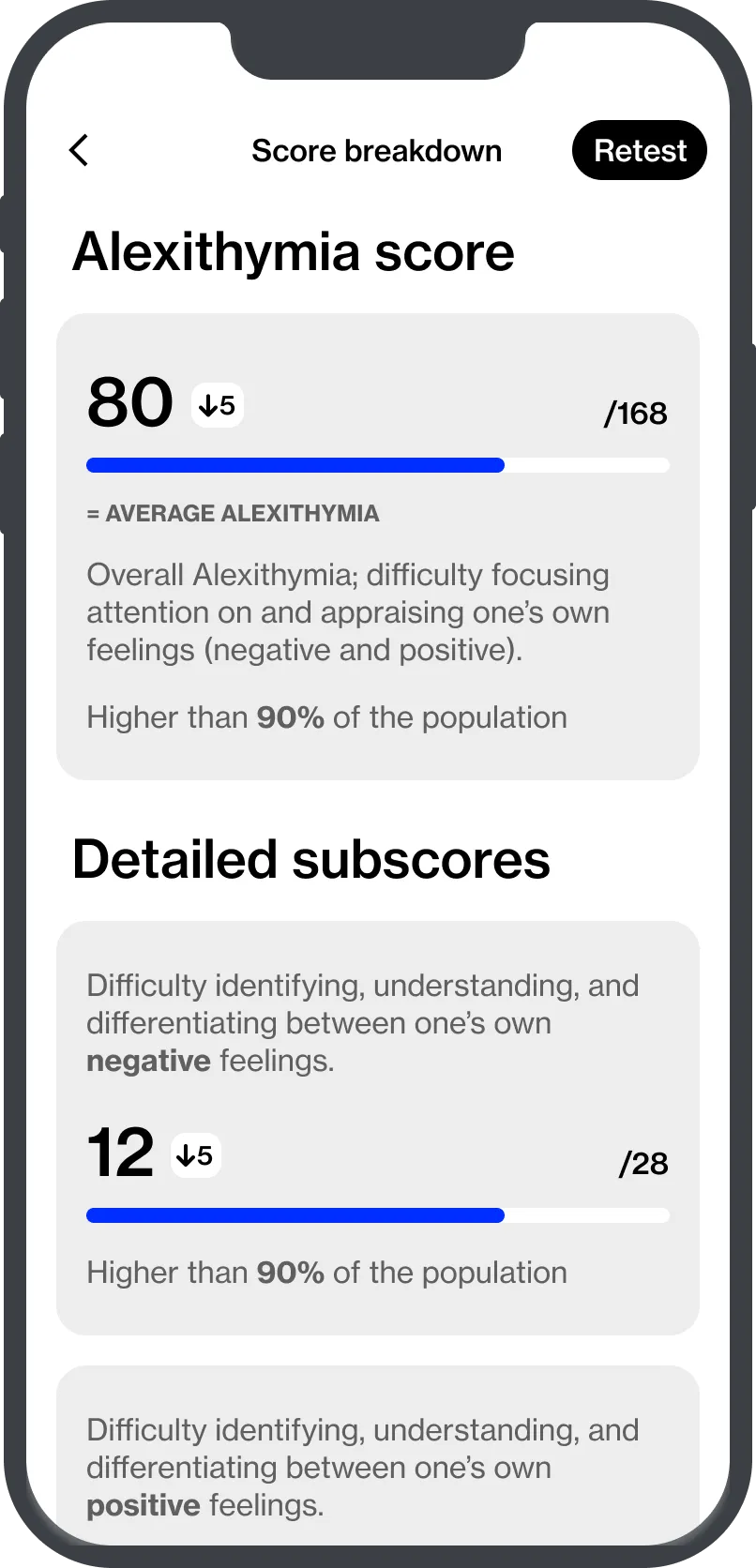
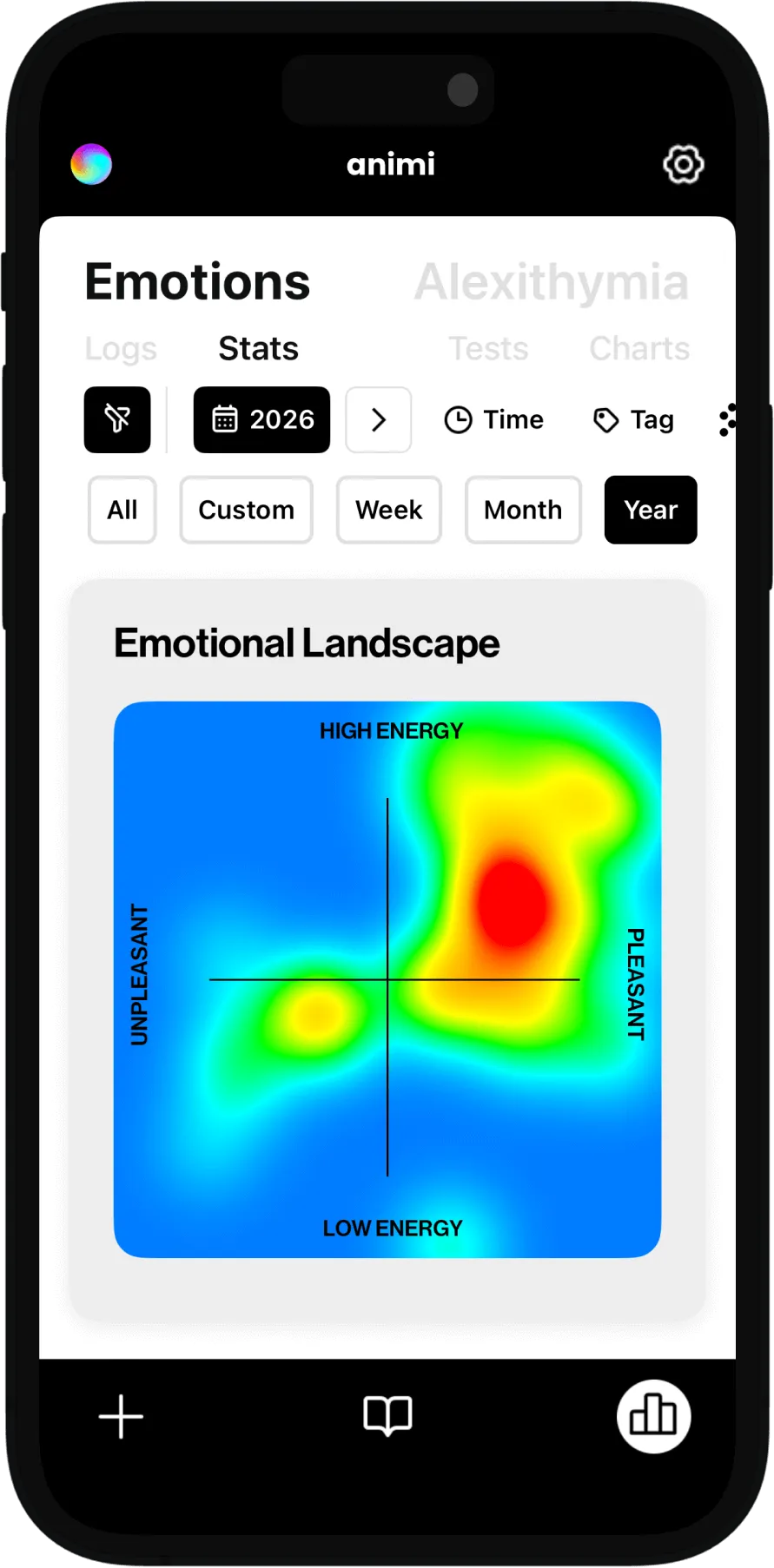
- Take the alexithymia test to get a baseline and track change over time.
- Work through Emotions 101 course if you want guided, structured practice.
References
- Luminet O, Nielson KA. Alexithymia: Toward an experimental, processual affective science with effective interventions. Annu Rev Psychol. 2025;76:741-769. doi:10.1146/annurev-psych-021424-030718.
- Bagby RM, Parker JDA, Taylor GJ. The twenty-item Toronto Alexithymia Scale-I. Item selection and cross-validation of the factor structure. J Psychosom Res. 1994;38(1):23-32. doi:10.1016/0022-3999(94)90005-1.
- Salminen JK, Saarijarvi S, Aarela E, Toikka T, Kauhanen J. Prevalence of alexithymia and its association with sociodemographic variables in the general population of Finland. J Psychosom Res. 1999;46(1):75-82. doi:10.1016/S0022-3999(98)00053-1.
- Kinnaird E, Stewart C, Tchanturia K. Investigating alexithymia in autism: a systematic review and meta-analysis. Eur Psychiatry. 2019;55:80-89. doi:10.1016/j.eurpsy.2018.09.004.
- Kiraz S, Gul H, Askin R, Gamsizkan Z. The relationship between alexithymia and impulsiveness in adult attention deficit and hyperactivity disorder. Psychiatry Investig. 2021;18(8):754-761. doi:10.30773/pi.2020.0414.
- Kivimaki V, Kuitunen-Paul S, Salokangas RKR. Association between alexithymia and substance use: A systematic review and meta-analysis. Scand J Psychol. 2022;63(5):427-438. doi:10.1111/sjop.12821.
- Westwood H, Kerr-Gaffney J, Stahl D, Tchanturia K. Alexithymia in eating disorders: Systematic review and meta-analyses of studies using the Toronto Alexithymia Scale. J Psychosom Res. 2017;99:66-81. doi:10.1016/j.jpsychores.2017.06.007.
- Li S, Zhang B, Guo Y, Zhang J. The association between alexithymia as assessed by the 20-item Toronto Alexithymia Scale and depression: A meta-analysis. Psychiatry Res. 2015;227(1):1-9. doi:10.1016/j.psychres.2015.02.006.
- Hemming L, Haddock G, Shaw J, Pratt D. A systematic review and meta-analysis of the association between alexithymia and suicide ideation and behavior. J Affect Disord. 2019;254:34-48. doi:10.1016/j.jad.2019.05.011.
- Aaron RV, Finan PH, Wegener ST, Keefe FJ, Lumley MA. Alexithymia in individuals with chronic pain and its relation to pain intensity, physical interference, depression, and anxiety: a systematic review and meta-analysis. Pain. 2019;160(5):994-1006. doi:10.1097/j.pain.0000000000001487.
- Ogrodniczuk JS, Piper WE, Joyce AS. Effect of alexithymia on the process and outcome of psychotherapy: a programmatic review. Psychiatry Res. 2011;190(1):43-48. doi:10.1016/j.psychres.2010.04.026.
- Quilty LC, Taylor GJ, McBride C, Bagby RM. Relationships among alexithymia, therapeutic alliance, and psychotherapy outcome in major depressive disorder. Psychiatry Res. 2017;254:75-79. doi:10.1016/j.psychres.2017.04.047.
- Brewer R, Cook R, Bird G. Alexithymia, not autism, is associated with impaired interoception. Cortex. 2016;81:215-220. doi:10.1016/j.cortex.2016.03.021.
- Bagby RM, Taylor GJ, Parker JDA, Dickens SE. The development of the Toronto Structured Interview for Alexithymia: item selection, factor structure, reliability and concurrent validity. Psychother Psychosom. 2006;75(1):25-39. doi:10.1159/000089224.
- Preece DA, Becerra R, Robinson K, Gross JJ. The psychometric assessment of alexithymia: development and validation of the Perth Alexithymia Questionnaire. Pers Individ Dif. 2018;132:32-44. doi:10.1016/j.paid.2018.05.011.
- Mazza M, Marchetti D, Ferri F, Quattropani MC, Verrocchio MC. Identifying therapies to effectively reduce alexithymia: A systematic review and meta-analysis. Psychiatry Res. 2026;340:122642. doi:10.1016/j.psychres.2026.122642.
- Ricciardi L, Demartini B, Edwards MJ, Fotopoulou A. Alexithymia in neurological disease: A review. J Neuropsychiatry Clin Neurosci. 2015;27(3):179-187. doi:10.1176/appi.neuropsych.14070169.
- de Vroege L, Emons WHM, Sijtsma K, van der Feltz-Cornelis CM. Psychometric properties of the Bermond-Vorst Alexithymia Questionnaire (BVAQ) in the general population and a clinical population. Front Psychiatry. 2018;9:111. doi:10.3389/fpsyt.2018.00111.
- López-Muñoz F, Pérez-Fernández F. A history of the alexithymia concept and its explanatory models. Int J Environ Res Public Health. 2020;17(19):7233. doi:10.3390/ijerph17197233.
- Jørgensen MM, Zachariae R, Skytthe A, Kyvik KO. Genetic and environmental factors in alexithymia: a population-based study of 8,785 Danish twin pairs. Psychother Psychosom. 2007;76(6):369-375. doi:10.1159/000107565.
- Grabe HJ, Schwahn C, Barnow S, Spitzer C, John U, Freyberger HJ, et al. Alexithymia, hypertension, and subclinical atherosclerosis in the general population. J Psychosom Res. 2010;68(2):139-147. doi:10.1016/j.jpsychores.2009.07.015.
- Di Tella M, Ghiggia A, Tesio V, Romeo A, Colonna F, Fusaro E, et al. Alexithymia and hypertension: does personality matter? A systematic review and meta-analysis. Curr Cardiol Rep. 2023;25(12):1665-1680. doi:10.1007/s11886-023-01894-7.
- Tolmunen T, Lehto SM, Heliste M, Kurl S, Kauhanen J. Alexithymia is associated with increased cardiovascular mortality in middle-aged Finnish men. Psychosom Med. 2010;72(2):187-191. doi:10.1097/PSY.0b013e3181c65d00.
- Terock J, Klinger-König J, Janowitz D, Grabe HJ, Freyberger HJ, Spitzer C. Alexithymia is associated with increased all-cause mortality risk in men, but not in women: a 10-year follow-up study. J Psychosom Res. 2021;146:110472. doi:10.1016/j.jpsychores.2021.110472.
- Vadini F, Di Blasio A, Ciarapica D, Piersimoni D, Concetti C, Cioffi A, et al. Alexithymia and estimated 10-year cardiovascular disease risk in healthy adults: a community-based cross-sectional study. Front Psychol. 2024;15:1504143. doi:10.3389/fpsyg.2024.1504143.
- De Gucht V, Heiser W. Alexithymia and somatisation: a quantitative review of the literature. J Psychosom Res. 2003;54(5):425-434. doi:10.1016/S0022-3999(02)00467-1.
- Kano M, Muratsubaki T, Morishita J, Van Oudenhove L, Morikawa M, Dupont P, et al. Association between alexithymia and functional gastrointestinal disorders. Biopsychosoc Med. 2018;12:21. doi:10.1186/s13030-018-0134-3.
- Bećirović E, Avdibegović E, Softić R, Mirković-Hajdukov M, Bećirović A. Alexithymia in war veterans with post-traumatic stress disorder. Eur Psychiatry. 2017;41(S1):S720. doi:10.1016/j.eurpsy.2017.01.1301.
- Loas G, Speranza M, Pham-Scottez A, Perez-Diaz F, Corcos M. Alexithymia in adolescents with borderline personality disorder. J Psychosom Res. 2012;72(2):147-152. doi:10.1016/j.jpsychores.2011.11.006.
- Bøen E, Hummelen B, Boye B, Elvsåshagen T, Malt UF. Borderline patients have difficulties describing feelings; bipolar II patients describe difficult feelings. An alexithymia study. Acta Psychiatr Scand. 2020;142(3):203-214. doi:10.1111/acps.13204.
- The percentage and clinical correlates of alexithymia in stable patients with schizophrenia. The percentage and clinical correlates of alexithymia in stable patients with schizophrenia. BMC Psychiatry. 2023;23:207.
- Sequeira AS, Silva B. A comparison among the prevalence of alexithymia in patients with psychogenic nonepileptic seizures, epilepsy, and the healthy population: A systematic review of the literature. Psychosomatics. 2019;60(3):238-245. doi:10.1016/j.psym.2019.02.005.
- Prevalence and associated factors of alexithymia among people living with HIV/AIDS in China: a cross-sectional study. Prevalence and associated factors of alexithymia among people living with HIV/AIDS in China: a cross-sectional study. Front Psychiatry. 2023;14:1203824. doi:10.3389/fpsyt.2023.1203824.
- Pei JH, Wei YT, Tao HX, Yang QX, Zhang GL, Guo XJ, et al. The prevalence and characteristics of alexithymia in patients with type 2 diabetes mellitus: A systematic review and meta-analysis. J Psychosom Res. 2022;162:111018. doi:10.1016/j.jpsychores.2022.111018.
- Faidiga MR, Judeikis GA, Nisihara R, Skare TL. Alexithymia in systemic lupus erythematosus: A cross sectional study in a Brazilian sample. Lupus. 2023;32(1):80-86. doi:10.1177/09612033221139788.
- Ayache SS, Chalah MA. Alexithymia in multiple sclerosis: past, present and future. Front Hum Neurosci. 2025;19:1552494. doi:10.3389/fnhum.2025.1552494.
- Chimenti MS, Fonti GL, Conigliaro P, Hitaj J, Triggianese P, Teoli M, et al. Evaluation of alexithymia in patients affected by rheumatoid arthritis and psoriatic arthritis: A cross-sectional study. Medicine (Baltimore). 2019;98(4):e13955. doi:10.1097/MD.0000000000013955.
- Kallitsounaki A, Williams DM. Brief report: An exploration of alexithymia in autistic and nonautistic transgender adults. Autism Adulthood. 2023;5(2):180-186. doi:10.1089/aut.2022.0113.
- Nummenmaa L, Glerean E, Hari R, Hietanen JK. Bodily maps of emotions. Proc Natl Acad Sci U S A. 2014;111(2):646-651. doi:10.1073/pnas.1321664111.
- Preece DA, Gross JJ. Defining alexithymia: The clinical relevance of cognitive behavioral vs psychoanalytic conceptualizations. Pers Individ Dif. 2024;228:112732. doi:10.1016/j.paid.2024.112732.
- @violetxoxox. YouTube comment on alexithymia and therapy. YouTube. Accessed April 20, 2026.
- Sudden_Silver2095. Alexithymia is so much more than not…. Reddit r/AutismInWomen. 2024.
- Kanojia A. Therapist explains why you don’t feel anything anymore… (Alexithymia 101). HealthyGamerGG. November 3, 2022.
- Levant RF. The normative male alexithymia hypothesis. In: Levant RF, Pryor S, eds. Assessing and Treating Emotionally Inexpressive Men. Routledge; 2025.
- Mancini VO, Ditzer J, Brett JD, Gross JJ, Preece DA, et al. Internalizing symptoms in men: The role of masculine norms, alexithymia, and emotion regulation. Sex Roles. 2025;91:71. doi:10.1007/s11199-025-01615-0.
- Levant RF. Interview on normative male alexithymia and stress. Video interview. December 30, 2024.